Management of Terminal Edentulism by Implant-Supported Fixed Prostheses- A Case Report
<p style="text-align: justify;">What therapeutic attitude should be adopted in case of medium or extended terminal edentulism?. This clinical situation requires assessing the alternatives for the replacement of missing teeth. The therapeutic solutions available for this type of edentulism may be the implant-supported fixed prosthesis or the removable prosthesis. The conventional removable partial prosthesis does not satisfy all of our patients, considered unesthetic and often uncomfortable. However, the implant-supported fixed prosthesis is a solution that has proven to be satisfactory in terms of comfort, longevity and esthetics. A complete and successful implant treatment is based on an integrated approach consisting of two treatment phases, the surgical phase and the prosthetic one.</p>
Debbabi Imen1*, Harzallah Belhassen2, ben khelifa Mohamed3,
Troudi Fethi4 and Cherif Mounir5
Medicine Monastir, Tunisia
Tel: +21627430478; Email: debbabiimen@yahoo.fr
phases, the surgical phase and the prosthetic one.
Prosthetic Rehabilitation
Introduction
In the context of an oral implant rehabilitation, the purpose of the treatment is to provide a prosthesis placed on implants. The planning of a surgical implant treatment must therefore be preceded by a prosthetic study [1]. The objective of the implant planning is to choose the number, length, diameter and positioning of the implants. It results from the analysis of all the elements collected by the dentist during the medical questionnaire, the clinical examination, the realization of the prosthetic project and the study of the radiographic elements [2]. The Progress of implantology and the techniques for increasing bone volume allow the treatment of all the classes of edentulism and propose fixed restorations in place of conventional removable appliances [3].
The indication fields of the implant-supported prosthesis are constantly expanding. They make it possible to avoid the removable partial prosthesis which is often undesired by the patients because of its removability [4]. A traditional therapeutic solution will be considered only if the implant-supported fixed prosthesis is counter-indicated. This counter-indication can be for several reasons: anatomical constraints, esthetic risks, occlusal risks, medical counter indications, financial counter indications [4, 5, 6]. In this article, we will present a clinical case treated with implant-supported prostheses. We will argue the chosen therapeutic solution and describe the implant plan. A case of unilateral mandibular posterior edentulism and extended maxillary terminal edentulism will illustrate this point.
Case Report
A 55-year-old patient consulted the Department of Fixed Prosthodontics at the Dental Clinic of Monastir to replace his missing teeth with fixed prostheses. His general health condition was good. The patient was motivated but he was a smoking person (30 cigarettes per day). The extra-oral examination revealed no pathology. The patient had a sufficient and rectilinear mouth opening. The intra-oral examination showed that he had a poor oral hygiene, a lot of tartar, bacterial plaque, an inflammation of the dental papillae and the gingiva surrounding the defective right maxillary bridge. His attached gingiva was sufficient. It was equal to 3mm. His dental formula is as follows:
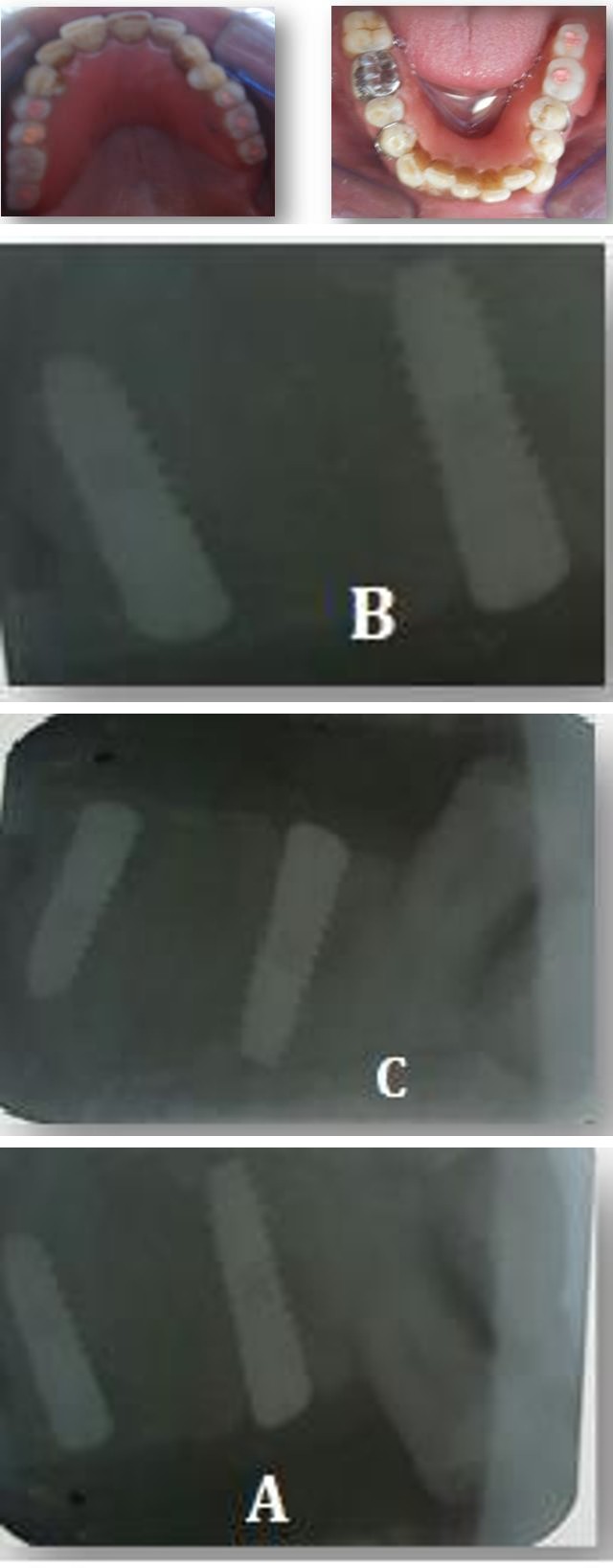
$$ \begin{array}{c c c c c c c c c c c c c c c} \mathbf {A} & \mathbf {A} & (6 & \mathbf {A} & 4) ^ {*} & 3 & 2 & 1 & 1 & 2 & 3 & 4 & \mathbf {A} & \mathbf {A} & \mathbf {A} & \mathbf {A} ^ {*} \\ \hline \mathbf {A} & 7 & (6) ^ {*} & 5 & 4 & 3 & 2 & 1 & 1 & 2 & 3 & 4 & 5 & 6 & 7 & 8 \end{array} $$ A* Missing tooth / ()*: Conventional fixed prosthesis: Crown /Bridge The dental examination revealed significant extrusion of the left mandibular molars reaching the antagonist alveolar crest, a slight egression of the # 47 and the presence of a maxillary three-unit veneered bridge (Figures 1 & 2). This bridge was very mobile.

Figure1: Closed mouth: right side. Figure 2: Closed mouth: left side.
The patient had a class I canine on the left side, a class I canine and molar on the right side and a non-retained Maximum Intercuspation position (MIP) and Vertical dimension of occlusion (VDO). Examination of the dynamic occlusion revealed a group functions in lateral movements on the working side without occlusal interferences and a dysfunctional anterior guidance. X-ray examination revealed important extrusion of the left mandibular molars and the presence of a bridge replacing the #15. The bridge had 2 retainers on premolar #14 and on the first maxillary molar#16 whose roots are much resorbed. The panoramic X-ray revealed generalized bone lysis reflecting chronic periodontitis (Figure 3).

Figures 3: Panoramic X-ray.
Pre-Implant Considerations
During the pre-implant phase we started by motivating the patient to improve his oral hygiene. Then, were moved the defective bridge and extracted its resorbed two retainers (#14 and #16). The left mandibular molars (#36 #37-#38) were also extracted. Later, the study casts were mounted on a semi-adjustable articulator in centric relation after having determined the patient’s correct VDO (Figures 4).
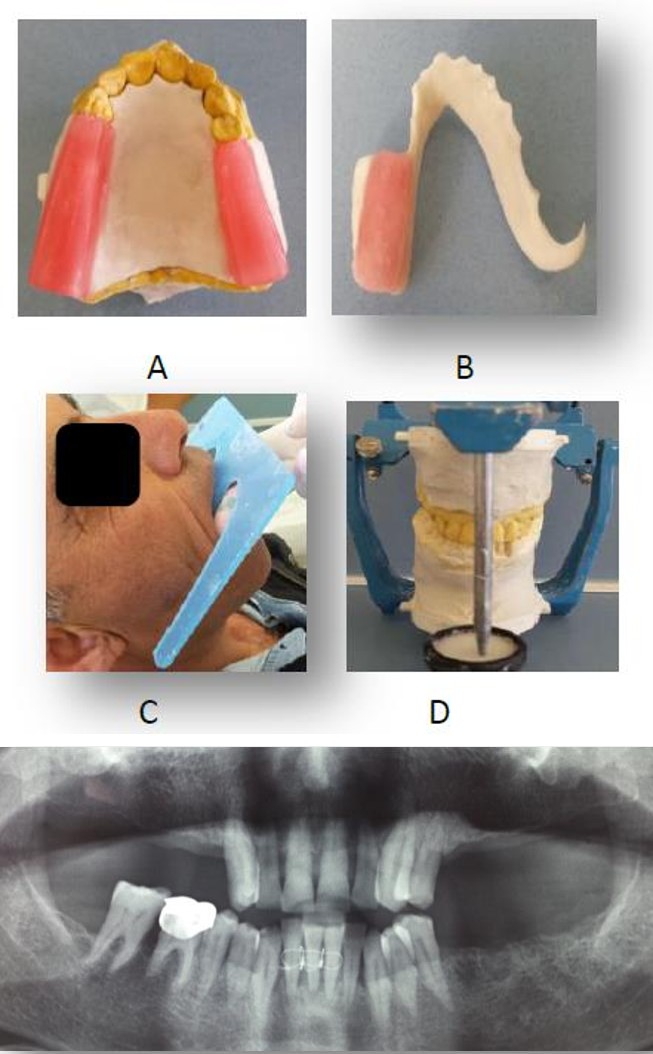
Figures 4: A: maxillary record base and wax rims; B: Mandibular record base and wax rim; C: Orientation of the upper occlusal plane using the occlusal plane guide (fox plane); D: Centric relation (CR) record The study models mounted on articulator allowed the analysis of occlusion, inter-arch relationship, prosthetic space available, and interferences, prematurity and occlusal pathologies [7]. The available prosthetic space was evaluated in the corono-apical and mesio-distal directions during the first clinical examination as well as during the analysis of the study models mounted on articulator [7]. In this case, the vertical prosthetic space assessed on articulator, following the extraction of the extruded teeth, was equal to 14mm on the left side and equal to 7mm on the right side. The patient later benefited of partial removable prostheses to restore the masticatory function. He was examined after six months to check bone healing. His oral hygiene improved and the periodontal disease, following the first non-surgical step, was stabilized (Figure 5). The patient reduced tobacco consumption (7 cigarettes per day).
Figures 5: Panoramic X- ray.
Radiological Examination
At this stage, the prosthetic project was defined with the patient’s consent. It was then necessary to study the foundations possibilities. The implants should be placed in order to finalize the prosthetic project. So, it was necessary to analyze the bone volume according to this project [8]. To do this, removable partial protheses were transformed into a radiological guide. We then performed gaps in the middle of the prosthetic teeth and then filled them with guttapercha (radio-opaque mark) (Figure 6). The radiological guide allowed the visualization of the implant simulation on the cone beam, the future implant sites in the three planes of space as well as the bone and
| Left side: 2 implants | ||
|---|---|---|
| Right side: 3 implants | ||
| Site of 14: 3.5/12mm | Site of 25: 4/12mm | Site of 36: 4/10mm |
| Site of 15: 3.5/12mm | Site of 27: 4/10mm | Site of 37: 4/10mm |
| Site of 17: 4/10mm |
Table 1: The Prosthetic Decision.

The prosthetic phase
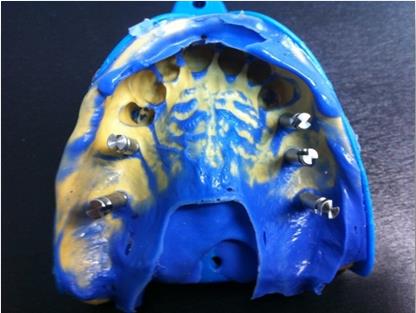
After 2 months, the prosthetic phase was initiated. In this case, impressions were taken using the direct technique known as pick-up technique. Later, they were sent to the dental laboratory (Figure 9).
The patient’s occlusion was recorded in centric relation (CR) using record base and wax rims. The metal frames were tested in the mouth and check-up X-rays

were taken to ensure their proper cervical adaptation (Figure 10). Then, the color was chosen.

The metal-ceramic fixed prostheses were tried in mouth (in a biscuit bake state) and the marginal fit, shade, shape and occlusion were evaluated. The static occlusion was controlled to check the bilateral distribution of the contacts at Maximum Intercuspation position (MIP) during maximum tightening. Dynamic occlusion was controlled to ensure the absence of interference .After Ceramic glaze, the prostheses were sealed using a temporary cement seal without eugenol ((Temp Bond NETM) (Figure 11).

Maintenance Phase
Periodontal and peri-implant maintenance is an essential step in the treatment plan [11]. It requires the patient’s permanent cooperation [12]. Its goal is to ensure the durability of our treatment, to prevent inflammatory reactions, loss of attachment and recurrence of periodontal disease [13]. Many studies have shown implant failure in patients who do not have regular follow up [14]. The frequency of the maintenance sessions depends on the risk factors that are according to Heitz- Mayfield: oral hygiene, history of periodontal diseases and smoking [15]. For Axelsson, et al. the maintenance frequency should be 2-4 times per year [13].
Discussion
Treatment of the posterior sector often represents the majority of the practitioner's implant activity. In private practice, 66.5% of posterior implants are reported [16]. Implant treatment of the posterior area presents few esthetic requirements. However, it can become problematic because of its anatomical and prosthetic characteristics [7]. Implants of the posterior sector are subjected to high occlusal constraints, up to 400% higher than those of the anterior sector [17]. Maxillary bone has a lower bone density than mandibular bone, especially in the posterior region. It is type IV. A good primary stability is more difficult to reach.
When edentulism is distal, the therapeutic choice will depend on the patient's request, the available bone volume and the available prosthetic space [7]. In the molar sector, large diameter implants can be placed when the width of the alveolar ridge allows. The replacement of premolars with standard implants and molars with wide implants makes it possible to better manage the problems of emergence profile, prosthetic morphology and occlusion. For posterior partial edentulism, the functional loads permit one implant per tooth. Increasing the number of implants reduces the occlusal constraints [7].
The crestal width measured at all the edentulous sectors in our case is ≤ 6 mm. In the edentulous areas where the width is equal to 6 mm, standard implants (3.75 to 4 mm) are used to replace premolars and # 27.In areas where the alveolar ridge is <6mm, a small diameter implant can be placed. When this path is chosen, implant placement is not dictated by the prosthetic imperative, it is the surgical imperative that dominates [7]. However, this compromise must lead to a prosthetically acceptable restoration since the placement of 3.5-diameter implants often leads to a difficulty in managing the spaces between elements as well as the emergence profile [7]. In this case, the approach chosen was to adapt to the available bone volume. Implants were placed without a bone augmentation procedure or alteration of bone morphology. For our patient, we chose two implants of reduced diameter (3.5mm) in the right maxillary sector to replace the # 14 and the # 15.
Flapless access has clinical benefits during and after surgery (Table 2) [7]. However, this technique was criticized for the risk of introducing epithelial and connective tissue residues into the implant osteotomy, which may compromise osseointegration, perforation of bone tables during "blind" drilling, and failure to obtain the desired implant axis. As a result, flapless surgery is only relevant when the ridge is very wide and the surgeon is experienced.
| During surgery | After surgery |
|---|---|
| -Less traumatic for the patient; | |
| -Absence of surgical mark; | |
| -Preservation of the gingival architecture of adjacent teeth; | -Minimal postoperative follow-up (bleeding, edema, pain); |
| -Less uncomfortable for the patient; | -Less risk of surgical wound infection; |
| -Reduced duration of surgery. | -Less manipulation of soft tissues; |
| - Minimal cervical bone loss; | |
| -optimized osseointegration; | |
| -Optimized esthetic result. |
Table 2: Clinical benefits of flapless access during and after surgery [7].
The Pick-up impression technique provides the greatest precision according to a recent literature review [18, 19]. Polyvinyl siloxane impression materials offer increased working time, better ease of removal than polyethers because they are less rigid and they tear at a stage where permanent deformation is minimal. However, it is often necessary to use the same material with two different viscosities [20]. A vertical prosthetic space, bigger than or equal to 7 mm (from the neck of the implant up to the opposing tooth), is required for a sealed prosthetic restoration. This is the minimum space to be able to place the abutment and the crown [7].
Conclusion
Prosthetic rehabilitations with implant-supported prostheses have fewer counter-indications. However, the removable partial prosthesis always finds its indications. It is necessary to respect the design, biomechanical, esthetic and occlusal requirements to obtain a satisfactory result. The removable partial prothesis may constitute a transient therapy preceding an implant-supported fixed therapy. The removable prosthesis then plays an essential role in the implant bed conditioning during the temporization period, following avulsions. The practitioner must master the prosthetic check phase to offer the patient psychic comfort, to protect implants and to guide gingival healing. He must know how to implement it without making errors that could affect his goal.
Acknowledgement: Special thanks to Mr. Boukattaya Samir for the revision of the English grammar and syntax errors.
References
-
Lamy M (2011) Prothèse implantaire fixe scellée et vissée à l’heure du numérique. L’information dentaire pp: 12-23: 1-6.
-
Diss A, Peltier B, Berdoug M (2009) La planification implantaire. Le Fil Dentaire 43: 45-48.
-
Simonet P, Exbrayat P, Missika P, Taddéi C, Limbour P, et al. (2011) Deux “Prothèse implanto-portée JSOP n°6.
-
Fouilloux I, Begin M (2007) Prothèse amovible versus prothèse fixe implanto-portée: Quelles indications ?. Réalités cliniques 18(3): 263-274.
-
Renouard F, Rangert B (2005) Prise de décision en pratique implantaire. Quintessence International pp: 209.
-
Walton JN, Mac Entee MI (2005) Choosing or refusing oral implants: A retrospective study of edentulous volunteers for a clinical trial. Int J Prosthodont 18(6): 483-488.
-
Davarpanah M, Szmukler-Moncler S, Rajzbaum Ph, Davarpanah K, Demurashvili G (2012) Manuel d’implantologie clinique. Concepts, intérgration des protocoles et esquisse de nouveaux paradigmes. 3rd (Edn.).
-
Lamy M (2013) Planification du plan de traitement implantaire: le projet prothétique. Implant 19: 35-43.
-
Patrick Goudot, Jean-Pierre Lacoste (2013) Guide pratique d'implantologie. 1st (Edn.), pp: 248.
-
Benhamou A, Kleinfinger (2007) Etude pré prothétique pré implantaire. Le Fil Dentaire 24: 20- 21.
-
Hassaneyn S (2014) Maintenance en implantologie. Le Fil Dentaire 95: 29-30.
-
Abillama M, Sojod B (2013) La maintenance péri- implantaire. Le Fil Dentaire 85.
-
Axelsson P, Nyström B, Lindhe J (2004) The long term effect of aplaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. J Clin Periodontol 31(9): 749-757.
-
Pjetursson BE, Helbling C, Weber HP, Matuliene G, Salvi GE, et al. (2012) Péri implantitis susceptibility as it releates to periodontal therapy and supportive care. Chir Oral Implants Res 23(7): 888-894.
-
Heitz-Mayfield LJ (2008) Péri implant diseases: diagnosis and risk indicators. J Chir Periodontal 35 (8): 292-304.
-
Nedir R, Bischof M, Briaux JM, Beyer S, Szmukler- Moncler S, et al. (2004) A 7 year life table analysis from a prospective study on ITI implants with special emphasis on the use of short implants. Results from a private practice. Clin Oral Implants Res 15(2): 150- 157.
-
Anderson DJ (1956) Measurement of stress in mastication: I. J Dent Res 35(5): 664.
-
Lee YJ, Heo SJ, Koak JY, Kim SK (2009) Accuracy of different impression techniques for internal- connection implants. Int J Oral Maxillofac Implants 24(5): 823-830.
-
Y Benhamou, Y Allard, Y Charbit, P Mahler (2010) La prise d’empreintes en prothèse sur implants: problèmes et erreurs. Stratégie prothétique 10(4).
-
Degorce ET (2005) Empreinte implantaire et empreinte de prothèse fixée Quelle différence. Stratégie prothétique 5(1): 41-47.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey